
![]()
The intersection of eating disorders and competitive sports presents a critical issue that demands attention. Athletes, driven by the desire for peak performance and often subjected to intense physical and psychological pressures, are particularly vulnerable to developing eating disorders.
Dear Visitors,
Please find below a study that was published in nture.com, ‘Exploring the prevalence and risks of eating disorders in Lebanon’s athletic community’. We share this study for the research and information purposes only.
Exploring the prevalence and risks of eating
disorders in Lebanon’s athletic community
Scientific Reports volume 15, Article number: 8054 (2025)
Abstract
The intersection of eating disorders and competitive sports presents a critical issue that demands attention. Athletes, driven by the desire for peak performance and often subjected to intense physical and psychological pressures, are particularly vulnerable to developing eating disorders. The aim of our study is to conduct a preliminary assessment of the prevalence and risk levels of EDs among athletes in Lebanon. Using the validated EAT-26 and the DESA-6 questionnaires, 250 athletes were interviewed as part of a cross-sectional survey. Anthropometric measurements and sociodemographic characteristics were also assessed. The main findings show that the overall risk of EDs among Lebanese athletes is 21%, with 54.5% of those at-risk being males. In addition, the uncontrollable use of dietary supplements was observed in 41% of athletes. Being an adult aging 25 years and above, male, practicing sports for more than 5 years coupled with more than 15 h per week with post graduate diploma increases significantly ED risks. The prevalence of EDs among athletes in Lebanon is a well-recognized concern, highlighting the need for proactive measures and targeted interventions.
Introduction
Eating disorder (ED) is a mental health condition characterized by persistent disturbances in eating behaviors and related thoughts and emotions1. These disorders often involve preoccupation with food, body weight, and shape, leading to extreme behaviors that affect an individual’s health and well-being. There are several types of EDs that can affect the general population, including anorexia nervosa (AN), bulimia nervosa (BN), and binge eating disorder (BED)2. AN is characterized by an intense fear of gaining weight leading to severe food intake restrictions, and extreme affective symptoms3. This can result in dangerously low body weight, nutritional deficiencies, and other health and psychiatric complications4,5,6,7. BN involves cycles of BED followed by purging behaviors, such as self-induced vomiting or excessive exercise, to compensate for the consumed calories3. BED is denoted by recurrent episodes of consuming large amounts of food in a short period, often accompanied by feelings of loss of control4,5,6,7. ED is significant concern in the sports and fitness world, presenting athletes with unique challenges and pressures1. An athlete is an individual who is skilled in physical activities or sports, often participating in competitive events that require strength, speed, agility, endurance, and coordination. Athletes typically engage in rigorous training and practice to enhance their performance in specific sports or disciplines. They may compete at various levels, including amateur, collegiate, professional, or international levels, depending on their expertise and achievements. According to a recent systematic review on 70,957 athletes from both genders in 177 studies, one in five athletes is at a greater risk of developing an ED8. However, the prevalence in the Middle East, especially in Jordan, is higher (34%), whereby gymnastics (10%) and taekwondo (8%) contributing the most to EDs9. The serious consequences of competing with an eating disorder include decreased strength, endurance, and concentration, which can lead to suboptimal performance and increased risk of injury8,9Research supports the serious consequences of competing with an eating disorder, highlighting its impact on physical performance, cognitive function, and injury risk. Athletes with eating disorders often experience significant energy deficits, which can impair strength and endurance. For example, athletes with low energy availability have been found to have a 2.5 times higher risk of fatigue and reduced physical performance (OR = 2.5, 95% CI: 1.7–3.6)10. Additionally, cognitive function scores, including attentional capacity, were significantly lower in athletes with disordered eating patterns, with a reported 40% reduction during high-intensity exercise11. Furthermore, the risk of stress fractures and overuse injuries is considerably higher in athletes with a history of disordered eating behaviors, with one study reporting a 4.5 times greater risk (RR = 4.5, 95% CI: 3.1–6.6)12. These findings underscore the severe physical and mental health risks associated with competing while managing an eating disorder. In addition, athletes in sports that emphasize weight-sensitive sports that prioritize leanness and endurance, appearance, or performance, such as gymnastics, figure skating, wrestling, combat sports13, and distance running, may be particularly vulnerable to developing ED14,15. While some athletes may engage in disordered eating behaviors to improve performance or gain muscle mass, others, specifically females, may do so to meet weight requirements or fit certain aesthetic ideals14,15,16,17. Gender differences in ED among athletes have been well documented in research studies17. While both male and female athletes can be affected by ED, there are some notable differences in the prevalence and presentation of these disorders. For example, female athletes are more likely to experience ED such as AN and BN, often driven by societal pressures to maintain a certain body image17,18,19. On the other hand, male athletes may be more prone to muscle dysmorphia or excessive exercise as a means of controlling their weight17,18,19. The global rates of disordered eating patterns and ED range from 0 to 19% among male athletes and 6–45% among female athletes19. To our knowledge, research on ED among athletes has been scarce in the Middle East, especially related to incidence and prevalence. A few studies have been conducted in Jordan, Saudi Arabia, and Iran8,9,20,21,22. Therefore, the aim of our study is to have a primary assessment of the level of EDs and ED risks among athletes in Lebanon.
Materials and methods
Study design and sampling procedures
This cross-sectional study was carried out between June and October 2022. Eligible participants aged 18–64 years were enrolled in this study using a convenient sampling approach. Athletes who are practicing any type of sports were invited to participate in this study through their national sports federations, following an introduction of the study’s objective. Athletes meeting the eligibility criteria and expressing interest in participating were encouraged to complete a self-administered online questionnaire. The study design is demonstrated in Fig. 1.
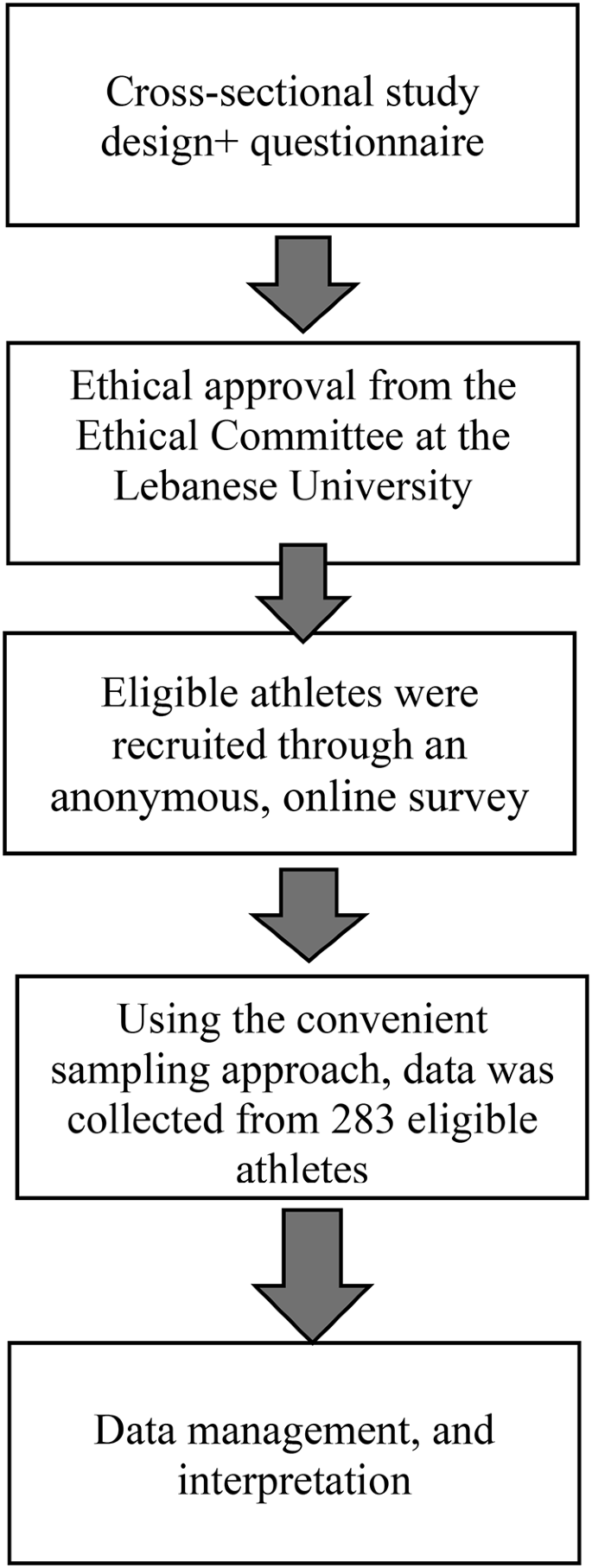
Flowchart of the study design.
Participants
A sample size of 250 participants was determined using the Kish and Leslie formula to achieve a statistical power exceeding 80%23. Anticipating a non-response rate of 10%, a total of 300 athletes were initially included in the study. Ultimately, a response rate of 94% was achieved. To be eligible for participation, athletes had to be at least 18 years old, Lebanese citizens, and officially affiliated with Lebanese sports federations based in Beirut. All eligible athletes consented to participate in the study upon contact. The sampled population consisted of both professional and amateur athletes who had been engaged in their respective sports for a minimum of 2 years. The distinction between professional and amateur athletes lies in their compensation, commitment, and competition levels. Professional athletes receive financial compensation for their participation in sports, including salaries, prize money, and endorsements, and playing sports their primary career24. In contrast, amateur athletes typically do not earn income from sports, participating instead for personal development or passion while balancing athletics with other responsibilities, such as education or work25. Professional athletes dedicate significant time and resources to training and compete at elite levels, such as professional leagues and international events, while amateurs often compete in local, regional, or collegiate events26. Additionally, eligibility rules often distinguish between the two groups; for example, amateur athletes may be restricted from professional leagues or compensated competitions to maintain fairness in events like the Olympics27. These differences highlight the varying roles sports can play in individuals’ lives, from a recreational activity to a full-time career. Among the 261 athletes, 60% were men and 40% were women. More than 90% of the athletes competed at the national level. On average, the study recruited 283 athletes across four sports categories: 55.2% were involved in ball games (football, basketball, handball, etc.), 11.9% in combat sports (taekwondo, karate, judo, etc.), 24.9% in endurance sports (running, swimming, cycling), and 8% in weightlifting/bodybuilding. The participants were selected through convenient sampling. The dependent variable in the study was the occurrence of ED, while the independent variables encompassed participant demographic characteristics (age, sex, level of education), duration and type of sports practice, the level of competition.
Study Instruments related to ED
EDs were assessed using the Eating Attitudes Test (EAT) that was validated in Arabic28,29,30. The Disordered Eating Screen for Athletes (DESA-6) was also used31. Using the validated EAT-26 and DESA-6 as the base of the self-administered questionnaire, a section covering sociodemographic factors, and health-related aspects, including age, gender, nationality, weight, height, marital status, address, monthly household income, and employment status was added. Moreover, dietary supplement use was assessed. Another section included inquiries about sports involvement, such as years of sports practice, types of sports, weekly exercise duration, competition level, ranking, and more. EAT 26 consists of 26 items and utilizes a 6 –point Likert scale ranging from 1 (never) to 6 (always). Scores at or above 20 on the EAT-26 indicates potential risk for eating disorders. As for the scoring of the screening tool DESA-6 A positive score of ≥ 2 on the DESA-6 is considered indicative of potential eating disorder prevalence32. The full questionnaire was translated to Arabic using the method of forward translation and back translation.
Ethical considerations
Our research was carried out following ethical approval from the Ethical Committee at the Lebanese University (#43/January 6, 2022). The questionnaire’s introductory page included a consent form, ensuring the anonymity and non-traceability of participants’ responses. Participation in the study was entirely voluntary, and participants were informed of their option to withdraw at any time. Informed consent was obtained from all individual participants included in the study.
Statistical analysis
Data collected from the survey questionnaire were coded and analyzed using Stata statistical software release 12 (Stata Corporation). Descriptive statistics were used to describe the general characteristics of the whole sample and after stratified by gender. For continuous variables such as height and weight the mean and standard deviation (SD) were used, and for categorical variables like BMI category and education level, numbers and proportions were stated. An independent two-sample t-test and Pearson chi-square test was used to test the differences between men and women in their general characteristics. Factors associated with EAT-26 among Lebanese adults were assessed using cross-tabulation and chi2 statistical tests to compare the differences in the proportion between adults at risk of ED or not at risk of ED. Furthermore, a binary logistic regression model-1, with the “at risk of ED” as a dependent variable, was then used to determine the variables that independently predicted the risk of having an eating disorder. The model was adjusted for age, gender and BMI. In addition, factors associated with DE were investigated, using a chi2 test to assess differences in the proportion of adults at risk of DE based on DESA-6 scores. Furthermore, a logistic regression (model-2) with “at risk of DE” as the dependent variable was used to determine the variables that independent predictors of this risk. Model-2 was adjusted for age, gender and BMI. Findings were assessed by the odds ratio (OR) and 95% CI. A statistical significance level of p < 0.05 was used.
Results
Sample characteristics
A total of 261 participants were included in this study, of whom 64% were men. The mean age of the total sample was 33 ± 10 years old. There were significant differences between men and women in their average height and weight. Although men had higher BMI by 0.95 kg/m2 than women, there was no significant difference between them (95%CI: −1.9 to 0.01; p < 0.053). Table 1 illustrates participants’ general characteristics. Most of the study participants were single (52.5%), followed by married (43%) and the differences were significant (p < 0.021). In terms of employment status, 46.7% of the total sample were full time employee, and this proportion was higher in males than in females (55.4% and 31.6% respectively), with a significant difference (p < 0.000). Only 13% of the total sample had chronic diseases, and 68% of them were females (p < 0.000). There was also a significant difference in the proportions of the type of chronic diseases (p < 0.000). However, there were no significant differences between males and females in the proportion of educational level or household income level (Table 1).
Dietary supplement use among athletes
Table 2. shows the consumption of dietary supplements among Lebanese adult athletes participating in this study. Only 41% reported consuming dietary supplements. There was a significant difference in supplement use between men and women (p = 0.023), while there are no significant differences between genders in the types of dietary supplements used.
Participant’s sport experience
Table 3 illustrates participants’ sport experience and characteristics. Ball games was the most common sport practiced by both men and women, flowed by endurance sports (63%, 41.7% and 15.8%, 40.6% respectively). However, there were significant differences between men and women in the type of the sports they routinely practiced. Additionally, significant gender differences were found in the years of practicing sport and sport ranking (amateur and professional) (p = 0.000 and p = 0.045, respectively).
Prevalence of ED and its associated risk among Lebanese adult athletes
Assessment of EDs using EAT-26
Figure 2 shows participants’ responses to EAT 26 questions. 91% of participants reported good self-control around food, while 73% enjoyed trying new rich food and 68% of participants also indicated a fear of being overweight. Table 4 demonstrates the prevalence of ED among the total participants and by gender. In total, there were 21% (95% CI: 16%, 27%) of participants who was at risk of ED, 54.5% (95% CI: 40.5%, 68%) of whom were males and 45.5% (95% CI: 32%, 59%) were females. 6% of the participants classified as underweight according to their age and gender. Regarding behavioral questions that represent possible ED symptoms or recent significant weight loss, 48% of the participants answered one or more questions. There were no significant differences between males and females in the score of EAT-26 or BMI (underweight) or behavioral questions.

Participants responses to EAT-26.
Assessment of DEB using DESA-6
Assessing ED using DESA-6 among Lebanese adults’ athletes revealed that there is 45.5% of participants were identified as at risk for ED. While 36% of those at risk were women and 64% were men, there were no statistically significant differences in ED prevalence between genders based on DESA-6 scores (p = 0.663). This finding was consistent even after adjusting for potential confounding factors like age and BMI with an odds ratio of 0.89 (95% CI: 0.53, 1.48; p = 0.649). Table S1 illustrates responses to DESA-6 questions (Table 4).
Determinants of eating disorders among Lebanese adult athletes
Using EAT-26
Table 5 illustrates factors associated with EAT-26 score. Findings show that adults aged 25 years old and above were more likely to have a higher risk of ED by an OR of 2.4 (95% CI: 1.1 to 5.1; p value = 0.029) than youth, after adjusting for gender, and BMI. While being male was less likely to have ED compared to being female (OR = 0.44; 95% CI: 0.21 to 0.91; p value = 0.029) after adjusting for confounders, significant differences were found in the proportion of partners’ education between participants with risk of ED and those without (p = 0.038). Furthermore, the total time participants spent in weekly exercise 9more than 15 h) was associated with the risk of ED, and this association was significant with and without adjusting for confounders (p = 0.022 and p = 0.038, respectively). No associations were found between participants’ education, occupations, household income, and type of sport with risk of ED.
Using DESA-6
Multiple factors were investigated to determine their association with DESA6 score among Lebanese adult athletes. This analysis was conducted using cross-tabulation and after adjusting for confounders. Findings showed no significant association between DESA6 and general characteristics (age group, gender, BMI, occupation, and household income). Only participants’ level of education was significantly associated with DESA6, and this association remained consistent before and after adjusting for confounders (p = 0.014 and p = 0.026) (Table 7).
Discussion
The prevalence of ED among athletes in Lebanon was found to be critical and alarming. The overall risk of ED among Lebanese athletes stands at 21%, revealing 54.5% of males and 45.5% of females falling under this risk. This comes in line with previous studies that have shown greater levels of body dissatisfaction and higher disordered eating symptoms among athletes32,33,34,35,36. One systematic review discovering the prevalence of disordered eating in athletes, highlighted strong evidence showing that athletes are at a higher risk of ED, especially those competing in lean sports37. Contrastingly, Kantanista et al.35, found that aesthetic sports athletes have a more positive body image compared to nonaesthetic athletes. It is notable to highlight that ED risk increases among individuals with higher levels of body dissatisfaction36. Consequently, sports activities where athletes compete in leanness at elite levels may be at a higher risk for developing ED32. In our study 6% of participants were classified as underweight based on their age and gender. Furthermore, in terms of behavioral indicators related to ED symptoms or recent substantial weight loss, 48% of participants answered one or more positive questions. Such disordered eating behaviors that include rapid weight loss, sweating, and water deprivation are viewed by athletes as integral to their sport discipline, where even coaches may encourage these behaviors32,33,34,35,36. The drive for thinness and leanness among athletes comes from their motivation to improve their sports performance, desire to enhance their physical appearance, and boost self-confidence33. Hence, athletes have higher general and sport-related body dissatisfaction36. The drive for leanness and thinness in certain sports activities, driven by the necessity to achieve a high level of performance and align to cultural ideals regarding an athletic body type, prompts female athletes to restrict their diets, which in return is culminating the development of ED. Moreover, one of the symptoms of eating disorders is compulsive excessive exercise38, and as seen in this study, the total weekly exercise duration was found to be correlated with the risk of ED, and this association remained significant both with and without adjusting for confounders. In terms of dietary supplement consumption, our study shows that 41% of athletes take dietary supplements. This high prevalence of supplement use is concerning as it has been linked to an increased risk of eating disorders39. Athletes may turn to supplements in an effort to enhance performance or achieve an ideal body type, which can lead to disordered eating behaviors. Therefore, it is crucial to address the underlying factors contributing to both supplements use and the risk of eating disorders in this population39. While it is commonly observed that younger athletes generally face a greater risk of ED in comparison to adults36, our study revealed that adults aged 25 years and above were 2.4 times more likely to be at a higher risk of ED, after adjusting for age, gender, and BMI, compared to youth. Regardless of BMI, Rousselet et al.33explained that although BMI is an important somatic criterion in the screening of ED, lacks specificity when applied to athletes. However, higher BMI is often correlated to higher body dissatisfaction40,41. Further delving into the results of this study, men have a lower likelihood of having ED compared to women, after adjusting for confounders. Supported by Krebs et al.42, women are at higher risk of ED. However, it is important to mention that both women and men athletes are at higher risk of ED compared to the general population42. This higher risk might be influenced by a combination of several factors that include psychological, sociocultural, and biological3343,. All in all, the association between being male, over the age of 25, and engaging in sports for more than 5 years with an increased risk of ED could be attributed to various factors. For males, there has been growing recognition of the pressure to conform to specific body ideals, especially in sports where lean body mass and muscularity are valued. This pressure may lead to disordered eating behaviors, even though eating disorders have traditionally been viewed as a female issue. For individuals over 25, the risks may be linked to longer exposure to competitive environments, where the emphasis on body composition and performance intensifies with age, particularly in endurance and aesthetic sports. Finally, athletes who have been in sports for more than 5 years might experience accumulated stress related to performance expectations, body image issues, and the pressures of maintaining peak physical condition over time.
One of the notable strengths is this study being among the pioneering research in Lebanon investigating ED among athletes using a validated ED risk assessment instrument. However, it is crucial also to acknowledge that this study has certain limitations. The use of the EAT-26 and DESA-6 questionnaires in our study comes with both strengths and limitations. The EAT-26 has been validated in Arabic, making it an appropriate and reliable tool for assessing disordered eating behaviors among Lebanese participants. However, the DESA-6 has not undergone validation in Arabic, which may limit its effectiveness in this context. Additionally, cultural factors, such as the Lebanese tradition of communal eating and a strong connection to family meals, may influence how respondents interpret the questions about food-related behaviors. These cultural differences could affect the accuracy of responses, particularly when it comes to body image perceptions and eating habits. In light of this, future studies should consider adapting the DESA-6 to better reflect Lebanese cultural norms and validating it in Arabic to ensure its reliability. The use of convenience sampling is a limitation as it may introduce bias and limit the generalizability of the findings. Selecting participants based on accessibility rather than randomization can result in overrepresentation of certain groups. Future research should consider probabilistic sampling to ensure greater representativeness and validity. Moreover, the small sample size of this study might have limited the extrapolation of the findings. Additionally, another limitation would be the lack of specificity in categorizing the athletes, or a set criterion for athlete categorization.
In conclusion, ED has been receiving increased attention among athletes, yet there remain considerable knowledge gaps regarding their prevalence. The prevalence of ED among athletes in Lebanon is a recognized concern, underscoring the need for proactive measures and targeted interventions. In terms of proactive measures and targeted interventions for Lebanese athletes, several strategies could be effective in addressing eating disorder (ED) risks. First, there is a need for educational programs focused on healthy body image, nutrition, and mental well-being. These programs could be integrated into training regimens to raise awareness among athletes, coaches, and support staff about the signs of EDs and the importance of balanced nutrition for performance.
Another important intervention could be the development of policies that prioritize mental health support within sports organizations. Establishing accessible mental health resources, including counseling and psychological support, would help athletes address body image concerns and stress related to performance. Moreover, creating a culturally sensitive framework for eating disorder prevention that incorporates Lebanese dietary practices and traditional food habits would be essential. Policies should aim to create a supportive environment where athletes feel comfortable discussing their challenges with food and body image without fear of stigma or discrimination.
Finally, implementing regular screening for ED risks in athletes, particularly those involved in weight-sensitive or performance-driven sports, could help identify at-risk individuals early and provide them with the necessary support. These interventions, when tailored to the unique cultural and social context of Lebanon, could significantly reduce the incidence of eating disorders among Lebanese athletes.
Data availability
All data generated or analyzed during this study are included in this published article and its supplementary information in Table S1.
References
-
Marí-Sanchis, A., Burgos-Balmaseda, J. & Hidalgo-Borrajo, R. Eating disorders in sport. Update and proposal for an integrated approach. Endocrinol. Diabetes Nutr. 69 (2), 131–143 (2022).
-
Kalindjian, N., Hirot, F., Stona, A. C., Huas, C. & Godart, N. Early detection of eating disorders: a scoping review. Eat. Weight Disord. 27 (1), 21–68 (2022).
-
Mattar, L., Huas, C., Duclos, J., Apfel, A. & Godart, N. Relationship between malnutrition and depression or anxiety in Anorexia Nervosa: a critical review of the literature. J. Affect. Disord. 132 (3), 311–318 (2011).
-
Donato, K. et al. Gene variants in eating disorders. Focus on anorexia nervosa, bulimia nervosa, and binge-eating disorder. J. Prev. Med. Hyg. 63 (2 Suppl 3), E297–E305 (2022).
-
Mattar, L., Huas, C., EVHAN group & Godart, N. Relationship between affective symptoms and malnutrition intensity in severe Anorexia Nervosa. PLoS One. 7 (11), e49380 (2012).
-
Mattar, L., Thiebaud, M. R., Huas, C., Cebula, C. & Godart, N. Depression, anxiety and obsessive-compulsive symptoms in relation to nutritional status and outcome in severe anorexia nervosa. Psychiatry Res. 200 (2–3), 513–517 (2012).
-
Hoteit, M. et al. Prevalence, correlates, and gender disparities related to eating disordered behaviors among health science students and healthcare practitioners in Lebanon: findings of a national cross sectional study. Front. Nutr. 9, 956310. https://doi.org/10.3389/fnut.2022.956310 (2022). PMID: 35928833; PMCID: PMC9345498.
-
Ghazzawi, H. A. et al. A systematic review, meta-analysis, and meta-regression of the prevalence of self-reported disordered eating and associated factors among athletes worldwide. J. Eat. Disord. 12 (1), 24 (2024).
-
Ghazzawi, H. A. et al. The prevalence of at Risk Eating disorders among athletes in Jordan. Sports (Basel). 10 (11), 182 (2022).
-
Angeliki, M. et al. Relative Energy Deficiency in Sport (REDs): endocrine manifestations, pathophysiology and treatments. Endocr. Rev. 45 (Issue 5), 676–708. https://doi.org/10.1210/endrev/bnae011 (October 2024).
-
Ackerman, K. E. et al. Low energy availability surrogates correlate with health and performance consequences of relative Energy Deficiency in Sport. Br. J. Sports Med. 53 (10), 628–633. https://doi.org/10.1136/bjsports-2017-098958 (2019). Epub 2018 Jun 2. PMID: 29860237.
-
Tenforde, A. S. et al. Association of the Female Athlete Triad Risk Assessment Stratification to the development of bone stress injuries in Collegiate athletes. Am. J. Sports Med. 45 (2), 302–310 (2017). Epub 2016 Dec 30. PMID: 28038316.
-
Langan-Evans, C. et al. The psychological and Physiological Consequences of Low Energy Availability in a male Combat Sport Athlete. Med. Sci. Sports Exerc. 53 (4), 673–683 (2021).
-
Mancine, R. P., Gusfa, D. W., Moshrefi, A. & Kennedy, S. F. Prevalence of disordered eating in athletes categorized by emphasis on leanness and activity type – a systematic review. J. Eat. Disord. 8, 47 (2020).
-
Gusfa, D., Mancine, R., Kennedy, S., Bashir, D. A. & Saffarian, M. The relationship between disordered eating behaviors and injury rates in adolescent athletes. Int. J. Eat. Disord. 55 (1), 131–134 (2022).
-
Paixão, C., Oliveira, S. & Ferreira, C. A comprehensive model of disordered eating among aesthetic athletic girls: exploring the role of body image-related cognitive fusion and perfectionistic self- presentation. Curr. Psychol. 40 (11), 5727–5734 (2021).
-
Prnjak, K., Jukic, I., Tufano, J. J. & Perfectionism Body satisfaction and dieting in athletes: the role of gender and Sport type. Sports (Basel). 7 (8), 181 (2019).
-
Joy, E., Kussman, A. & Nattiv, A. 2016 update on eating disorders in athletes: a comprehensive narrative review with a focus on clinical assessment and management. Br. J. Sports Med. 50 (3), 154–162 (2016).
-
Bratland-Sanda, S. & Sundgot-Borgen, J. Eating disorders in athletes: overview of prevalence, risk factors and recommendations for prevention and treatment. Eur. J. Sport Sci. 13 (5), 499–508 (2013).
-
Gargari, B. P., Khadem-Haghighian, M., Taklifi, E., Hamed-Behzad, M. & Shahraki, M. Eating attitudes, self-esteem and social physique anxiety among Iranian females who participate in fitness programs. J. Sports Med. Phys. Fit. 50 (1), 79–84 (2010).
-
Khatib, M. A., Aljaaly, E. A., Hafiz, M. S., Alamri, A. & Alzahrani, W. The risk of low energy availability among athlete females in Saudi Arabia: a cross-sectional study. Front. Public. Health. 12, 1411724 (2024).
-
Al-Jumayan, A. A., Al-Eid, N. A., AlShamlan, N. A. & AlOmar, R. S. Prevalence and associated factors of eating disorders in patrons of sport centers in Saudi Arabia. J. Family Community Med. 28 (2), 94–102 (2021).
-
Kish, L. Survey Sampling. Am. Pol. Sci. Rev. 59 (4), 1025 (1965).
-
Hardin, M. & Hardin, B. Distinguishing professional and amateur athletes: compensation and organizational policies. Sports Manage. Rev. 7 (3), 200–215. https://doi.org/10.1016/S1441-3523(04)70031-7 (2004).
-
Coakley, J. Sports in Society: Issues and Controversies 12th edn (McGraw-Hill Education, 2017).
-
Loland, S. Fair play in Sport: A Moral norm System (Routledge, 2002). First published 2002 by Routledge 11 New Fetter Lane, London EC4P 4EE.
-
International Olympic Committee (IOC). Olympic eligibility rules and amateurism. (2020). Retrieved from https://www.olympic.org/. accessed on July 7, 2024.
-
Haddad, C. et al. Validation of the arabic version of the eating attitude test in Lebanon: a population study. Public. Health Nutr. 24 (13), 4132–4143 (2021).
-
Uriegas, N. A., Winkelmann, Z. K., Pritchett, K. & Torres-McGehee, T. M. Examining eating attitudes and behaviors in Collegiate Athletes, the Association between Orthorexia Nervosa and Eating disorders. Front. Nutr. 8, 763838 (2021).
-
Garner, D. M. & Garfinkel, P. E. The Eating attitudes Test: an index of symptoms of anorexia nervosa. Psychol. Med. 9 (2), 273–279 (1979).
-
Kennedy, S. F. et al. Initial validation of a screening tool for disordered eating in adolescent athletes. J. Eat. Disord. 9 (1), 21 (2021).
-
Kong, P. & Harris, L. M. The Sporting body: body image and eating disorder symptomatology among female athletes from leanness focused and nonleanness focused sports. J. Psychol. 149 (2), 141–160 (2015).
-
Rousselet, M. et al. Disordered eating in French high-level athletes: association with type of sport, doping behavior, and psychological features. Eat. Weight Disord. 22 (1), 61–68 (2016).
-
Lichtenstein, M. B. et al. Behind the athletic body: a clinical interview study of identification of eating disorder symptoms and diagnoses in elite athletes. BMJ Open. Sport Exerc. Med. 8 (2), e001265 (2022).
-
Kantanista, A. et al. Body Image of Highly Trained Female Athletes Engaged in Different Types of Sport. Biomed Res Int. ; 2018:6835751. (2018).
-
Borowiec, J., Banio-Krajnik, A., Malchrowicz-Mośko, E. & Kantanista, A. Eating disorder risk in adolescent and adult female athletes: the role of body satisfaction, sport type, BMI, level of competition, and training background. BMC Sports Sci. Med. Rehabil. 15 (1), 91 (2023).
-
Rizk, M. et al. Phys. Activity Eat. Disorders: Syst. Rev. Nutrients, ; 12(1):183. (2020).
-
Dittmer, N., Jacobi, C. & Voderholzer, U. Compulsive exercise in eating disorders: proposal for a definition and a clinical assessment. J. Eat. Disord. 6, 42 (2018).
-
Nagata, J. M. et al. Appearance and performance-enhancing drugs and supplements, eating disorders, and muscle dysmorphia among gender minority people. Int. J. Eat. Disord. 55 (5), 678–687 (2022).
-
Nath, S., Bhattacharya, S., Golla, V. B. & Kumar, R. Effect of Social Media on Diet, Lifestyle, and performance of athletes: a review of current evidence. Curr. Nutr. Rep. 13 (2), 240–250 (2024).
-
Karr, T. M., Davidson, D., Bryant, F. B., Balague, G. & Bohnert, A. M. Sport type and interpersonal and intrapersonal predictors of body dissatisfaction in high school female sport participants. Body Image. 10 (2), 210–219 (2013).
-
Krebs, P. A., Dennison, C. R., Kellar, L. & Lucas, J. Gender Differences in Eating Disorder Risk among NCAA Division I Cross Country and Track Student-Athletes. J Sports Med (Hindawi Publ Corp). ; 2019:5035871. (2019).
-
de Bruin, A. P. & Oudejans, R. R. D. Athletes’ body talk: the role of contextual body image in eating disorders as seen through the eyes of elite women athletes. J. Clin. Sport Psychol. 12 (4), 675–698. https://doi.org/10.1123/jcsp.2018-0047 (2018).
Ethics declarations
Competing interests
The authors declare no competing interests.
Funding Declaration
This research received no external funds.
Human ethics and consent to participate declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.”
Consent to participate statement
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
{kind=link}